INTRODUCTION
Esthetics is of prime concern to almost every individual. With the increased awareness and changing times, people seeking dental treatment for esthetic purpose has significantly increased. Hence, it has become important to have techniques and materials that can meet patients' esthetic desires, and also simultaneously provide the most conservative way to meet structural, biological, and mechanical requirements that can provide a long-term clinical durability.1
Veneers, since their introduction in 1938, have become one of the most predictable, esthetic, and least-invasive modalities of treatment. They demonstrate excellent clinical performance in terms of strength, longevity, conservative nature, and biocompatibility.2 They provide the dentist and the patient an opportunity to enhance patient's esthetics in a minimally invasive to virtually noninvasive way.3
CASE REPORT
A 25-year-old male patient presented to the Department of Conservative Dentistry and Endodontics for the treatment of discolored upper front teeth and malformed upper front left tooth. Patient's major concern was improvement of esthetics.
Complete history of the patient along with preoperative photographs was taken, and a diagnostic wax was made. The patient's medical and family history was noncontributory.
On clinical examination, it was found that patient had fluorosis (Fig. 1A) (Scale 5, severe fluorosis, Dean's Index) with peg lateral maxillary left lateral incisor (Fig. 1B). Following a detailed clinical examination and careful evaluation of the objective parameters of the patient's smile, it was found that ceramic veneers were best suited for the condition, as they provide the advantage of preservation of most of the natural tooth structure while achieving the esthetics along with the correction of malformed tooth (peg lateral). Six anterior maxillary veneers were required.
Prior to beginning of teeth preparation, the shade selection was done using vita shade guide and incisal guidance was checked. The shade for cervical and middle third was designated as A2 and incisal third as B1. A conservative preparation (full veneer with incisal-lapping preparation design) of the enamel was performed by using a 0.5-mm depth cutting bur on the buccal wall, starting from the gingival level moving toward the incisal edge. The lingual margin was placed above the contact point. Dual convergence was given on the labial surface to preserve the anatomical form of the labial surface.
A long tapered chamfer-ended diamond bur was used to reduce the buccal wall to create definite gingival and interproximal finishing line angles. The chamfer was taken slightly into the interproximal areas so as to allow the veneers to cover all the visible aspects of the teeth.
After completion of the teeth preparation (Fig. 2), at the same appointment, the impression was made. Gingival displacement was obtained using retraction cord (#000, Ultradent). The retraction cords were removed and the impression was made with putty silicone (polyvinyl siloxane impression material) (Fig. 3), and an occlusal registration was made.



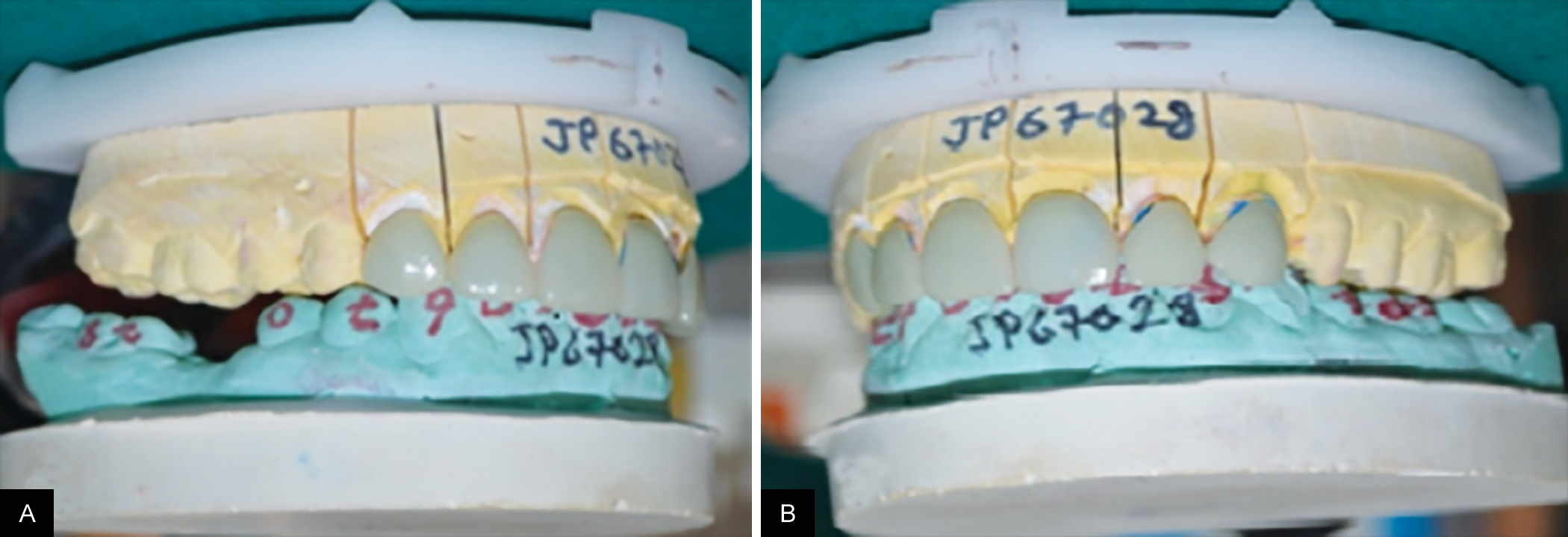
The impression was sent to the lab along with the instructions regarding the underlying and final shades, the desired length, and width and position of the frontal teeth. At the dental laboratory, refractory stone models of the prepared teeth were made, and six porcelain veneers were fabricated (Lithium disilicate IPS e. Max Press, Ivoclar, Vivadent). The six veneers were inspected in the dental office prior to the final placement in the patient's mouth (Figs 4A and B). Fit, marginal adaptation, appearance, translucency, shade, and the absence of the black triangle in the gingival area were checked. The try-in was done using glycerine medium. Following individual fitting, pairs, then groups of veneers were checked for proper contact, until all were properly related to one another. Each veneer was individually fitted and checked for marginal accuracy.
The teeth were then pumiced and rinsed. Then, enamel surfaces of the prepared teeth were etched using 37% phosphoric acid (Total Etch) for 15 seconds (Fig. 5A) followed by thorough rinsing with water spray for 20 seconds (Fig. 5B) and drying slightly. The adhesive agent was applied on the enamel (Fig. 5C) and photo-cured for 20 seconds using light curing system (3M, ESPE) (Fig. 5D). The internal surface of the veneers was etched with 10% hydrofluoric acid for 20 seconds (Condicionador de Porcelanos, Angelus). The surfaces were washed with water. The veneers were silanized with silane coupling agent (Silano, Angelus) (Fig. 5E). A total of 100% photocure resin cement (Variolink Veneer, Ivoclar, Vivadent) was used to cement the veneers to provide the highest color fidelity. The filled laminate was gently pressed to place and held there with a gloved finger while polymerizing with the light for 5 to 8 seconds (Fig. 5F). The initial excess cement was removed with the chisel end (Fig. 5G). Laminate was then completely cured for 60 seconds labially and lingually.
Figs 4A and B:
Checking the fit of the veeners on the cast: (A) Right lateral view; (B) left lateral view
Figs 5A to K:
Steps in cementation and polishing of the veeners: (A) Etching; (B) rinsing with water; (C) applying dentin bonding agent; (D) curing the bonding agent; (E) silanating the interior surface; (F) pressing the filled laminate and polymerising; (G) excess cement removed; (H) gingival reduction shaping or contouring managed with LVS - 7 micron diamond; (I) final smoothing and finishing with polishing cups; (J) rough interproximal areas smoothened using aluminum oxide using strips; and (K) abrasive disk used to polish incisal edges

Carbide-finishing burs were used to remove excess cured composite resin at the margins and make occlusal adjustments (Figs 5H and I). Any rough interproximal areas were smoothened using aluminum oxide polishing strips. Final smoothening and finishing was done with polishing cups and points (Figs 5J and K). Figures 6A to C present the intraoral view of six ceramic veneers from the facial, left, and right lateral aspect after cementation. Figure 7 shows a 6-month follow-up for the case.
DISCUSSION
One of the most frequent reasons patients seek dental care is discolored teeth. Even patients with teeth of normal color request whitening procedures. Treatment options include removal of surface stains, bleaching, microabrasion or macroabrasion, veneering, and placement of porcelain crowns.
Many dentists recommend porcelain crowns as the best solution for badly discolored teeth. If crowns are properly done with the highly esthetic ceramic materials currently available, they have great potential for being esthetic and long-lasting. On the contrary, there are increasing numbers of patients who do not want their teeth “cut down” for crowns and are electing an alternative, conservative approach, such as veneers that preserve as much of the natural tooth as possible.4
Figs 6A to C:
Postoperative intraoral view: (A) Front view; (B) left lateral view; (C) right lateral view


Veneer, which is a layer of tooth-colored material, is applied to a tooth to restore localized or generalized defects and intrinsic discolorations.
Direct and indirect laminate veneers have become popular treatment alternatives for patients with esthetic problems of anterior teeth in recent years.5
Bonded porcelain veneers provide a significant advantage of conservation of tooth structure, over metal–ceramic or all-ceramic crowns, which is a major factor in determining the long-term prognosis of any restorative procedure.6,7 They also provide a remarkable clinical durability, resulting in decreased potential pulpal involvement.8
Ceramics have predictable, esthetic, and long-lasting results. The procedure was intended to be minimally invasive; therefore, lithium disilicate ceramic veneers with thicknesses ranging from 0.3 to 0.5 mm were fabricated because they have relatively high wear resistance without compromising optical properties. The rehabilitation of smile esthetics with thin veneers is indicated to correct morphologic anomalies like the one done in this case, i.e., the correction of peg lateral.
CONCLUSION
Not too long ago people, be it common man or celebrities, wanted to show they have got a dental prosthesis with diamond studs or golden crowns or tooth jewelry. But now, bright, beautiful smiles are much in demand, and this is not just among celebrities, but ordinary people as well. They even consider them essential to social and business success. However, the proper understanding of the principles involved in fabrication of veneers and application is very important for the success of the treatment.9-11 A thorough clinical examination to assure the correct indication followed by a defined protocol is the major determinant of success. The aim of the dentist is not just to restore the esthetics, but to provide a restoration that provides the functional, biological, and mechanical integrity, thereby enhancing the general health and welfare of the patient.12,13